Stephen Costello
CEO & Co Founder
Our Approach to AI in Mental Health
Dev Diary — April 2026
One in four people will experience a mental health difficulty in any given year. The traditional system built to support them: therapists, counsellors, employee assistance programmes, was designed for a fraction of that number.
Waiting lists run months long. EAPs reach roughly 5% of the people they cover. Clinicians are stretched. And the gap between the number of people who need support and the capacity to provide it isn’t closing. It’s widening.
AI is the only way to change that equation. But not in the way most people assume.
We’re not building an AI therapist. We’re not replacing clinicians. We’re building a clinical AI ecosystem that extends what human care can reach, ensures quality across every session, and gives employers and insurers intelligence they’ve never had access to before.
This is how we’re doing it, and why each piece matters.
Augmented care, not automated care
Before anything else, a principle.
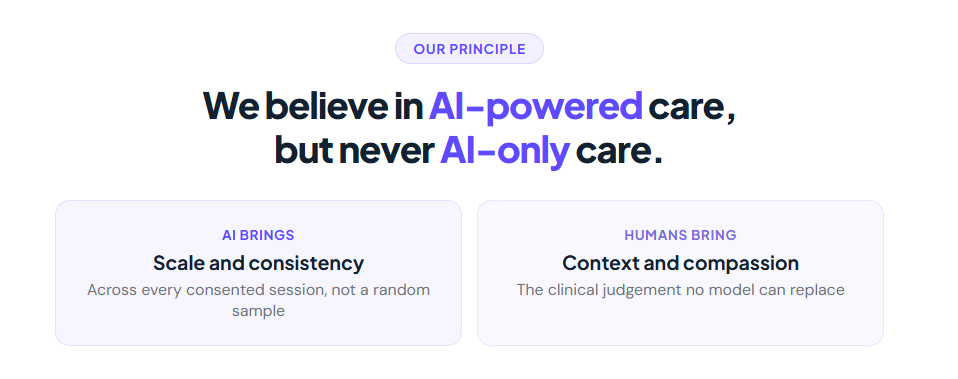
We believe in AI-powered care, but never AI-only care. AI brings scale and consistency. Humans bring context and compassion. Both are essential, and neither works without the other.
That sounds simple enough on paper. In practice, it only works if three groups of people trust it.
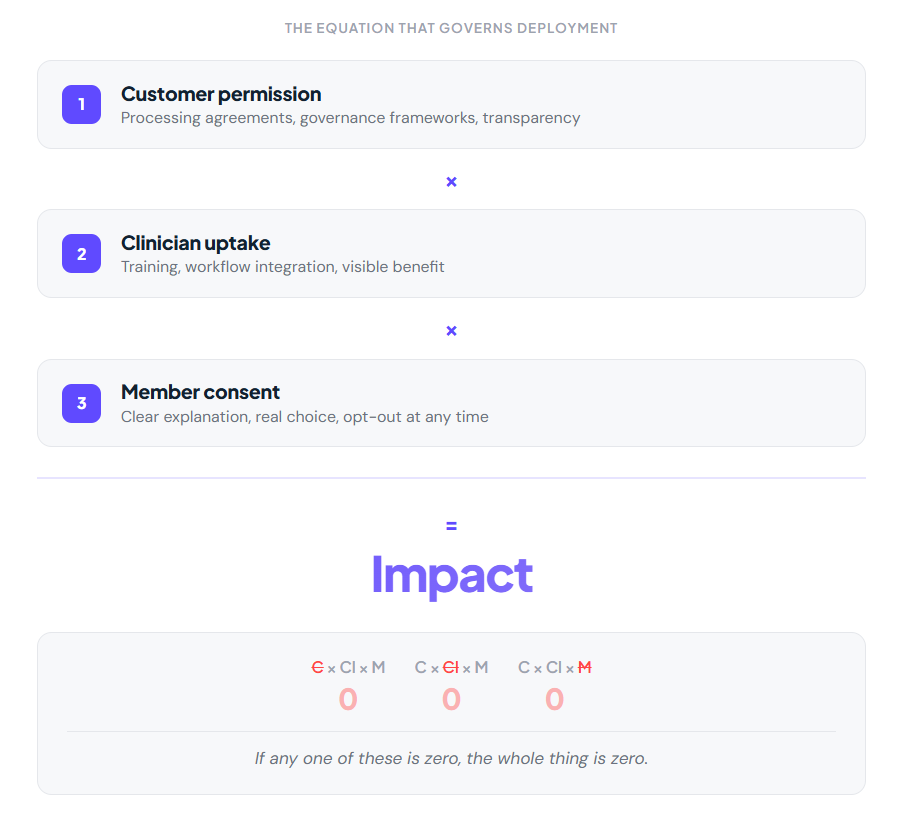
Customers have to grant permission. Whether that’s an SMB with 50 employees or an insurer with two million members, you earn the right to deploy AI on their population before you switch anything on. That means processing agreements, governance frameworks, and full transparency about what AI is doing and why.
Clinicians have to use it. Not tolerate it but use it. That means training, integration into how they already work, and design that respects established clinical workflows. If the tool creates friction, clinicians will work around it. They have to see and feel the benefit for themselves and for their clients.
Members have to consent. Not in the small print. Real, informed consent built on a clear explanation of what they get in return. A service user can opt out at any point.
Think of it as a formula: customer permission, multiplied by clinician uptake, multiplied by member consent, equals impact. If any one of those is zero, the whole thing is zero.
That equation governs everything we build.
The ecosystem: Four connected capabilities
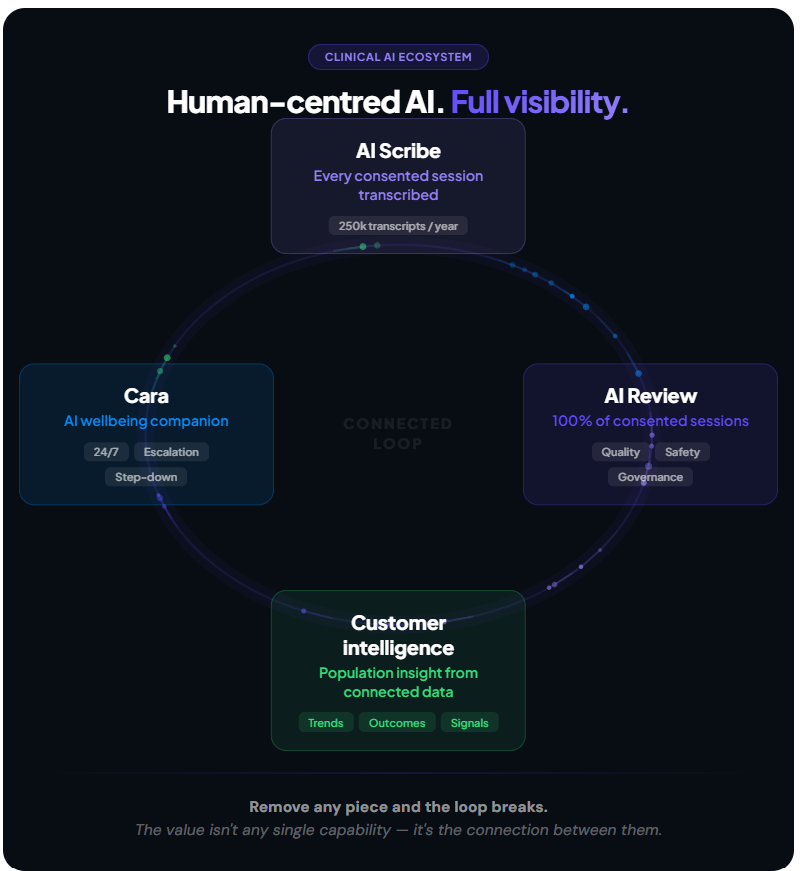
This isn’t one tool. It’s four capabilities that form a continuous loop across every clinical interaction we deliver.
AI Scribe transcribes every consented session in real time, approximately 250,000 per year across triage, support, and structured therapy. No audio is stored. No clinical data leaves our environment. The transcripts feed everything that follows.
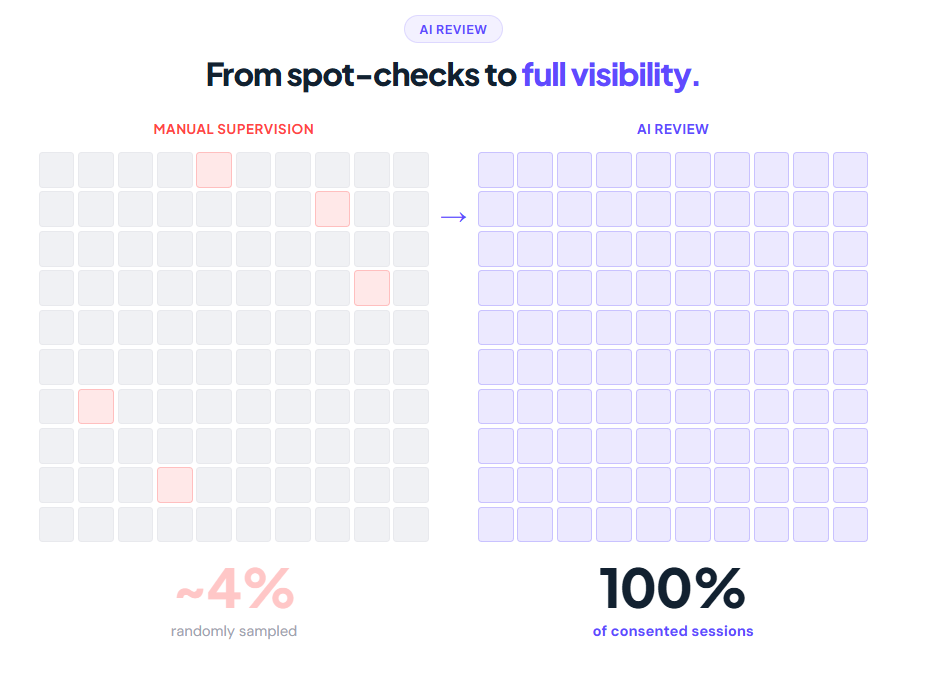
AI Review is our proprietary system. It takes every transcript and runs it through four structured agents aligned to best-practice supervision frameworks: clinical quality, safety and risk, consistency of practice, and governance. Most services review 2 to 5% of sessions. We have visibility across 100%. The output is a dashboard each clinician can use to see where they’re excelling and where they can strengthen their practice. Clinician development, not surveillance.
Cara is our AI wellbeing companion, always available, always on. Guided wellbeing, evidence-based emotional support, and deterministic escalation to our 24/7 clinical contact centre when risk is detected. 32% of conversations happen between 10 p.m. and 1 a.m. That’s demand the traditional system can’t serve. Cara Plus, a CE Class IIa medical device for anxiety and depression with a published RCT, is expected to achieve certification in early 2027.
Customer Intelligence turns all of this into population-level insight for employers and insurers. Not a quarterly utilisation report. Live, contextual intelligence, such as presenting issues, workplace signals, recovery rates, emerging risk, drawn from real clinical interactions and AI engagement data.
The connected loop: These four don’t sit in isolation. Transcripts feed the review. The review raises clinical standards. Cara catches people between sessions and before absence. Session context and Cara data combine to produce the intelligence layer. Remove any piece and the loop breaks. The moat isn’t any single capability, it’s the connection between them.
AI Review — from partial insight to full visibility
Clinical supervision is built on strong foundations — safe practice, clinician development, reflective space. A supervisor reviews sessions against structured competency frameworks, examining the therapeutic alliance, the interventions used, and adherence to evidence-based models.
It works well with a small team. At scale, it breaks down. Hundreds of clinicians. Thousands of sessions a week. Most services review 2 to 5% of them. The rest is never directly observed.
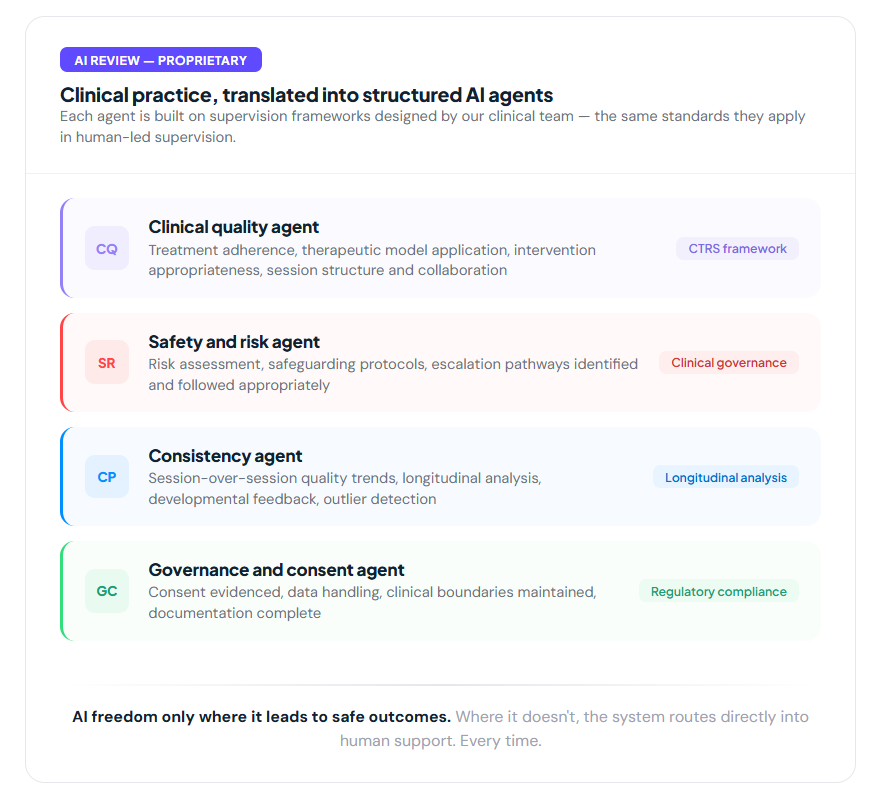
AI Review changes that. Every consented session transcript runs through four structured agents aligned to best-practice supervision agents:
- Clinical quality: therapeutic model application, collaboration, structure, interventions.
- Safety and risk: risk exploration, safeguarding, escalation pathways.
- Consistency: standards maintained over time, not just in isolated sessions.
- Governance: consent evidenced, boundaries maintained, documentation complete.
The output is a dashboard each clinician can see, where they’re excelling, where they can strengthen. Every flag links to a specific moment in the session.
Supervision stays relational, reflective, and developmental. AI Review adds earlier identification of learning needs, more targeted conversations, and consistent standards across the full team. Not surveillance. Development.
The shift: from a 4% sample to 100% of consented clinical activity.
The build: Clinical expertise is the engineering
There are many AI tools available today. The difficult part isn’t finding them, it’s making them work for clinical care. And that’s a clinical challenge before it’s a technical one.
We have 350 in-house clinicians and access to over 1,000 network clinicians. They’re not end users waiting for a product to land on their desk. They’re inside the engineering process, defining what good clinical practice looks like, building the supervision frameworks our AI agents are trained against, labelling the data, and catching the model when it gets something wrong.
That’s the difference between AI built for healthcare and AI built by people who deliver healthcare. Our clinicians translate years of therapeutic practice into the structured logic that powers AI Review. They design the escalation protocols that govern Cara. They validate that the output meets the same clinical standards they hold themselves to every day.
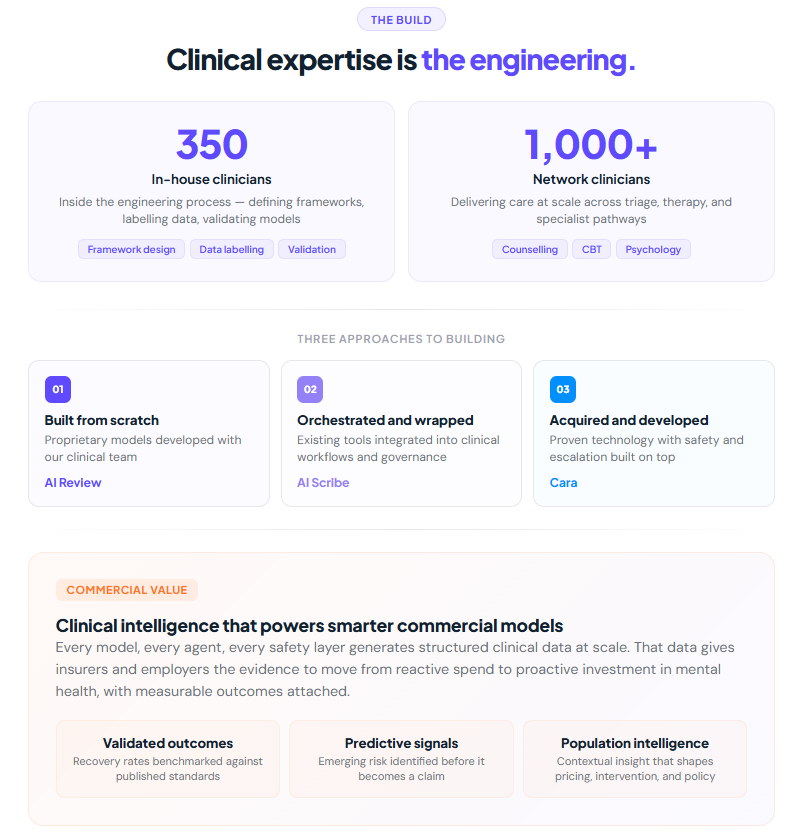
We take three approaches to building. Some tools are built from scratch, like AI Review is entirely proprietary, developed with our clinical team from the ground up. Some we orchestrate and wrap, such as AI Scribe, where the transcription technology exists but the integration into clinical workflows, consent processes, and quality assurance is all on us. Some we acquire and develop further, like Cara, where we took proven technology and built the safety architecture, clinical escalation, and intelligence layer around it.
What makes this commercially valuable is what sits behind the technology. Every model, every agent, every safety layer is grounded in real clinical practice delivered at scale. That’s what allows us to offer employers and insurers something they can trust, not AI as a concept, but AI governed by the same clinical standards that govern our human-delivered care. Same frameworks. Same accountability. Same outcomes measurement.
The other thing people get wrong is where to give AI freedom. In healthcare, that question has to be answered with absolute clarity. We test where giving the model freedom leads to safe outcomes. Where it doesn’t, the system routes directly into human support. Every time. That boundary isn’t a limitation, it’s the product.
What this means
We move from partial visibility to full insight into the care we provide. From delayed feedback to real-time clinical support. From reactive services to proactive care that identifies risk early and intervenes before it escalates.
For clinicians, better support. For supervisors, better insight. For clinical leaders, genuine assurance across the entire operation. For employers and insurers, confidence that care is safe, consistent, and effective, with the evidence to prove it.
And for the people who need support? Someone is always there. At two in the morning. Between appointments. Before it gets worse.
That’s the point. Not the technology for its own sake. The reach it creates.
This is Series 1 of 4. Next: Cara: what it does, how it works, and the clinical evidence behind it.